
Tonsils
Palate and Tonsil Surgery
The other airway levels that obstruct with OSA include the palate which we call the retropalatal (behind the palate) airway, and the retrolingual airspace (airway behind the tongue). The oral appliances can improve the retrolingual airway, but do little for the retropalatal airway. The palate contributes about 20% to sleep apnea, whereas, the retrolingual airway is responsible for approximately 80% of sleep apnea. Any surgical procedure must address all of these levels.
Surgery for the palate is very effective for snoring, but is only 50% effective for sleep apnea. This is because most people have retrolingual collapse in addition to retropalatal collapse, so surgery directed at the palate as the sole source of the problem is only partial treatment.
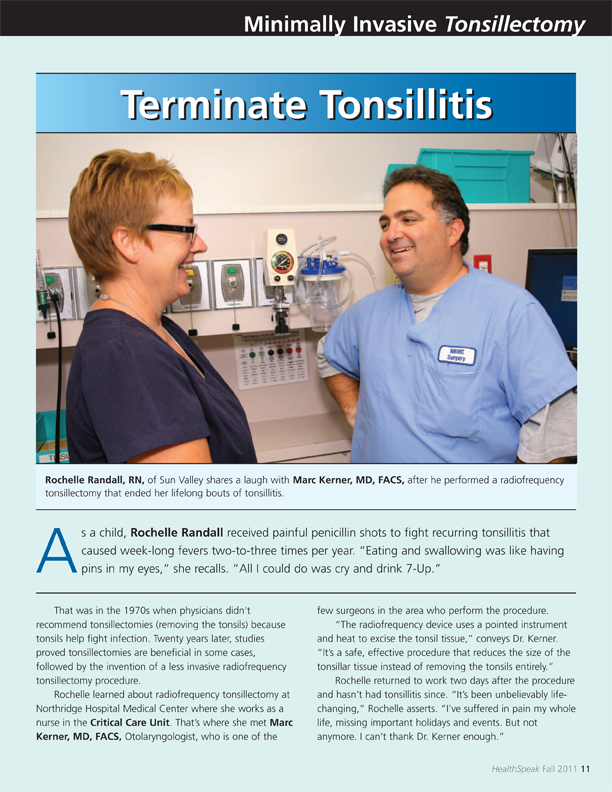
Procedures for the palate include a uvulopalatopharyngoplasty (UPPP), in which the soft palate is tightened, and tissue is removed to stiffen the palate. If tonsils are present, they are removed at the same time. For people with mild apnea and large tonsils we can approach this with radiofrequency technology. Dr. Kerner presented the largest series of minimally invasive tonsillectomy procedures at the American Academy of Otolaryngology meeting in September 2005. This is effective for reducing large tonsils and results in improved breathing and a reduction in throat infections.
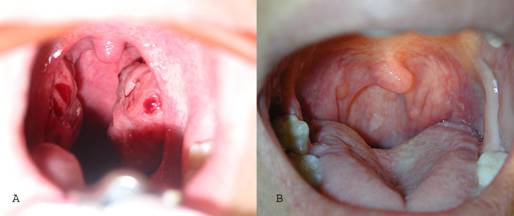
A-tonsils before radiofrequency B-Pharynx after radiofrequency tonsil reduction
When a palate surgery is indicated, Dr. Kerner utilizes the uvulopalatal flap. For patients with large tonsils, and a thick, elongated uvula, radiofrequency procedures are less effective so the more involved uvulopalatal flap with tonsillectomy is performed.