
According to the Sleep Disorders Guide (click here for the complete article)
The following are some statistics regarding this surprisingly common affliction.
- Sleep apnea is prevalent in as many as an estimated 18 million Americans alone. This statistic denotes that approximately 1 in every 15 Americans, or 6.62% of the total American population have a case of sleep apnea.
- Research conducted at the University of California's San Diego campus studied 54 African Americans and 346 Caucasians for the presence of sleep apnea. The results showed that a full 17 percent of African American test subjects had a case of obstructive sleep apnea present, compared to 8 percent of the Caucasian subjects. This denotes a hypothesis that African Americans stand an increased risk of obstructive sleep apnea.
- Two to four percent of all Americans have an undiagnosed case of sleep apnea. This accounts for approximately 1 in 50 individuals being undiagnosed.
- People that are afflicted with sleep apnea face a steep increase in chances of being part of a traffic accident. Due to the sleeplessness and lack of ability to concentrate that are associated with apnea, sufferers are six times more likely to die in a car accident. As a matter of fact, the National Highway Traffic Safety Administration has stated that drowsy driving is responsible for, at the very least, 100,000 car accidents, 40,000 injuries, and 1,550 deaths per year.
- More than 263,000 children per year undergo tonsillectomies. Most of these operations are performed due to the presence of sleep apnea in the children that is caused by the tonsils obstructing their air way.
- A bed mate of a person with untreated obstructive sleep apnea can lose a serious amount of sleep! Due to the breathing and gasping of the apnea sufferer, the bed mate loses up to an hour per night of sleep. This was discovered when a study was conducted that measured the effects of CPAP treatment in helping the bed mate to sleep.
- People that have an untreated case of sleep apnea face a risk of stroke that is four times as likely as those who are not afflicted. Untreated sleep apnea sufferers are also three times as likely to have heart disease.
- On the average night's sleep, a sufferer of obstructive sleep apnea may experience 60 apneas per hour. This accounts for an average of 400 apneas per night!
- Roughly half of all hospital patients that have a case of hypertension are also afflicted with sleep apnea. Conversely, around half of all sleep apnea sufferers face a diagnosis of hypertension.
- According to the National Commission on Sleep Disorders Research, approximately 38,000 deaths occur on an annual basis that relate to cardiovascular problems that in one way or another are connected to sleep apnea. These problems include high blood pressure, hypertension and stroke, among others. An estimated six million American residents suffer from sleep apnea that is moderate to severe and may necessitate a late night visit to the e=emergency room. Unfortunately a great many people do not, as previously mentioned, even realize that they suffer from sleep apnea. This number is somewhere around 500,000 individuals.
As these statistics show, sleep apnea is not a problem to be taken lightly. The risks of mortality faced by those with untreated obstructive sleep apnea are simply not worth it when you consider all the types of sleep apnea treatment available.
ADULTS
EXCESSIVE DAYTIME SLEEPINESS
DIFFICULTY STAYING AWAKE WHILE DRIVING, READING OR WATCHING TV
MORNING HEADACHES AND LETHARGY
DAYTIME IRRITABILITY
HEARTBURN AT NIGHT
LOUD SNORING
BED PARTNER NOTICES GASPING, CHOKING, OR LONG PAUSES IN BREATHING DURING SLEEP
CHILDREN
RESTLESS SLEEP
SNORING
WITNESSED BREATH STOPS
DEVELOPMENTAL DELAYS
BEHAVIORAL PROBLEMS INCLUDING SYMPTOMS OF HYPERACTIVITY, ATTENTION DEFICIT DISORDER
OBESITY
IF YOU CAN ANSWER YES TO A NUMBER OF THESE SYMPTOMS PLEASE CONTINUE:
Do you:
- snore every night?
- wake suddenly during the night perspiring, choking or gasping for air?
- wake in the morning with headaches or a sore throat?
- fight falling asleep during the day, at work or while driving?
- feel irritable, have memory loss or a lack of concentration each day?
- suffer with obesity, reflux or high blood pressure?
Sleep disorders are a silent epidemic affecting the world's population. The debilitating conditions of these disorders include insomnia, persistent sleep deprivation, restless legs syndrome and obstructive sleep apnea. Truly fortunate are those individuals who, over an average lifetime, will experience over 200,000 hours of restful sleep. But for more than one third of the population, each night becomes an endless battle of interruptions caused by lifestyle choices, work schedules or poor health.
It is well documented that disordered sleeping becomes progressively apparent as we age, with 40 percent of the adult population snoring. Chronic snoring is a major symptom of obstructive sleep apnea. Unfortunately, 80 to 90 percent of adults with clinically significant obstructive sleep apnea remain undiagnosed. The effects of sleep apnea are not limited to adults; mouth breathing is a red flag for obstructive sleep apnea among sleeping children.
Obstructive sleep apnea poses a threat to your life and has been clinically identified to produce morbid consequences to your body such as obesity, hypertension, heart attack, stroke, diabetes, depression, dementia and unexplained sudden death. Obstructive sleep apnea (OSA) is a syndrome characterized by periods of cessation of breathing (apnea) or decreases in airflow during sleep (hypopnea) that occur during sleep. The syndrome is defined by an apnea-hypopnea index (the number of apneas plus hypopneas divided by the number of hours asleep). The number is 5 or higher in association with excessive daytime sleepiness.
4 percent of men 30 to 60 years old, and 2 percent of women in this age group fit this criteria. Looking at larger studies, 24% of men have indexes greater than 5, and 9% of women have indexes greater than 5. The worse the syndrome, the higher the index, and in some cases the index can exceed 100. Risk factors for OSA include obesity, increased neck circumference, craniofacial abnormalities, hypothyroidism, and acromegaly.
Snoring is a symptom of sleep apnea, but not everyone who snores has the syndrome. Other disorders cause daytime sleepiness and include narcolepsy, periodic limb movement disorder, and circadian-rhythm abnormalities.
Clinically most people with sleep apnea snore loudly, grunt or struggle with breathing while sleeping, and this causes their bed partner to seek sleep in a different room. Partners will also note concern when they note long pauses in their bed partner's patterns of breathing during sleep which is characteristic of sleep apnea. People with sleep apnea also have daytime sleepiness or somnolence, headaches, irritability, inability to concentrate, and fatigue. There are a number of medical conditions that are associated with OSA. Systemic hypertension or high blood pressure, and other cardiovascular diseases are associated with sleep apnea. Patients with sleep apnea have a three-fold increase in the rate of motor vehicle accidents. This rate falls to normal controls when those people are placed on CPAP.
The primary reason to be treated is to improve your quality of life. The risk factors associated with prolonged sleep apnea are known but not quantified. Clearly the risk of motor vehicle accidents is increased, but the true risk of sudden death, stroke, or heart attack because of sleep apnea is still unknown.
Diagnosis
People at risk for sleep apnea include those that are obese, hypertensive (high blood pressure), habitual snorers, and hypersomnolent (sleepy). We can predict the severity of OSA based on a combination of factors. Neck circumference or body-mass index correlates with severity. Neck circumference measurements are adapted by adding 4 cm for patients with high blood pressure, snoring (3 cm), or choking or gasping (3 cm). A low probability exists if the adjusted score is less than 43 cm, intermediate probability (4 to 8 times more likely) with a circumference between 43 and 48 cm, and a high probability (20 times) with an adjusted circumference greater than 48 cm.
The signs and symptoms of obstructive and central sleep apneas overlap, sometimes making the type of sleep apnea more difficult to determine. The most common signs and symptoms of obstructive and central sleep apneas include:
- Excessive daytime sleepiness (hypersomnia)
- Loud snoring
- Observed episodes of breathing cessation during sleep
- Abrupt awakenings accompanied by shortness of breath
- Awakening with a dry mouth or sore throat
- Morning headache
- Difficulty staying asleep (insomnia)
Disruptive snoring may be a more prominent characteristic of obstructive sleep apnea, while awakening with shortness of breath may be more common with central sleep apnea.
Obstructive sleep apnea occurs when the muscles in the back of your throat relax. These muscles support the soft palate, the triangular piece of tissue hanging from the soft palate (uvula), tonsils and tongue.
When the muscles relax, your airway narrows or closes as you breathe in, and breathing momentarily cuts off. This may lower the level of oxygen in your blood. Your brain senses this inability to breath and briefly rouses you from sleep so that you can reopen your airway. This awakening is usually so brief that you don't remember it.
You can awaken with a transient shortness of breath that corrects itself quickly, within one or two deep breaths, although this is rare. You may make a snorting, choking or gasping sound. This pattern can repeat itself 20 to 30 times or more each hour, all night long. These disruptions impair your ability to reach those desired deep, restful phases of sleep, and you'll probably feel sleepy during your waking hours.
People with obstructive sleep apnea may not be aware that their sleep was interrupted. In fact, many people with this type of sleep apnea think they sleep well all night.
Central sleep apnea, which is far less common, occurs when your brain fails to transmit signals to your breathing muscles. You may awaken with shortness of breath or headaches. The most common cause of central sleep apnea is heart disease. People with central sleep apnea may be more likely to remember awakening than people with obstructive sleep apnea are.
When to seek medical advice
Consult your primary physician if you experience, or if your bed partner observes the following:- Snoring loud enough to disturb the sleep of others or yourself
- Shortness of breath that awakens you from sleep
- Intermittent pauses in your breathing during sleep
- Excessive daytime drowsiness, which may cause you to fall asleep while you're working, watching television or even driving
Many people don't think of snoring as a sign of something potentially serious, and not everyone who has sleep apnea snores. But be sure to talk to your doctor if you experience loud snoring, especially snoring that's punctuated by periods of silence.
Ask your doctor about any sleep problem that leaves you chronically fatigued, sleepy and irritable. Excessive daytime drowsiness (hypersomnia) may be due to other disorders, such as narcolepsy.
Your doctor may make an evaluation based on your signs and symptoms or may refer you to a sleep disorder center. Such an evaluation often involves overnight monitoring of your breathing and other body functions during sleep. Tests to detect sleep apnea may include:
Polysomnography
Polysomnography or a sleep study is the gold standard for assessing patients for sleep apnea. A quality sleep lab is the best method for obtaining the appropriate data, however, some home studies can be effective. Home oximetry can be correlative, a test in which patients are monitored for desaturation or a drop in oxygen saturation in the blood while sleeping. The sleep study gives us considerable data that allows us to fully evaluate the quality of sleep, and if necessary, with a CPAP (continuous positive airway pressure) titration study, we can determine what treatment parameters are required to reverse the apnea.
- Nocturnal polysomnography.
During this test, you're hooked up to equipment that monitors your heart, lung and brain activity, breathing patterns, arm and leg movements, and blood oxygen levels while you sleep. Because treatments for other sleep disorders such as narcolepsy and insomnia differ, this test helps your doctor to arrive at an accurate diagnosis.
- Oximetry.
This screening method involves using a small machine that monitors and records your oxygen level while you're asleep. A simple sleeve fits painlessly over one of your fingers to collect the information overnight at home. If you have sleep apnea, the results of this test will show drops in your oxygen level during apneas and subsequent rises with awakenings. If the results are abnormal, your doctor may have you undergo polysomnography to confirm the diagnosis. Oximetry doesn't detect all cases of sleep apnea, so your doctor may still recommend a polysomnogram even if the oximetry results are normal.
- Portable cardiorespiratory testing.
Under certain circumstances, you may be a candidate for a simplified test which can be performed at home to diagnose sleep apnea. These tests usually involve oximetry, measurement of airflow and measurement of breathing patterns.
If you are diagnosed with obstructive sleep apnea, you should be evaluated by an otolaryngologist who specializes in sleep apnea. An evaluation by a heart doctor (cardiologist) or a doctor who specializes in the nervous system (neurologist) may be necessary to look for causes of central sleep apnea.
Sleep apnea is a serious medical condition.
Complications may include:- Cardiovascular problems.
Sudden drops in blood oxygen levels that occur during sleep apnea increase blood pressure and strain the cardiovascular system. About half of people with sleep apnea develop high blood pressure (hypertension), which raises the risk of heart failure and stroke. If there's underlying heart disease, these repeated multiple episodes of low blood oxygen (hypoxia or hypoxemia) can lead to sudden death from a cardiac event.
The more severe the obstructive sleep apnea, the greater the risk for high blood pressure. A study published in November 2005 in the New England Journal of Medicine reported that obstructive sleep apnea greatly increases the risk of stroke, regardless of whether a person has high blood pressure. However, effectively treating obstructive sleep apnea can lower blood pressure and the risk of other cardiovascular diseases.
- Daytime fatigue.
The repeated awakenings associated with sleep apnea make normal, restorative sleep impossible. People with sleep apnea often experience severe daytime drowsiness, fatigue and irritability. They may have difficulty concentrating and find themselves falling asleep at work, while watching TV or even when driving. Children and young people with sleep apnea may do poorly in school or have behavior problems. The New England Journal of Medicine also published a study a number of years back which reported a significant increase in automobile accidents is people with sleep apnea compared to those without the condition.
- Complications with medications and surgery.
Obstructive sleep apnea also is a concern with certain medications and general anesthesia. People with sleep apnea may be more likely to experience complications following major surgery because they're prone to breathing problems, especially when sedated and lying on their backs. If you have diagnosed sleep apnea you should tell your doctor before you undergo general anesthesia. Undiagnosed sleep apnea is especially risky in this situation.
- Sleep-deprived partners.
Loud snoring can keep those around you from getting good rest and eventually disrupt your relationships. It's not uncommon for a bed partner to sleep in another room, or even on another floor of the house, to be able to sleep. Many bed partners of people who snore are sleep deprived as well.
People with obstructive and central sleep apneas may also complain of memory problems, morning headaches, mood swings or feelings of depression, a need to urinate frequently at night (nocturia), and impotence. Gastroesophageal reflux disease (GERD) is also more prevalent in people with sleep apnea. Children with untreated sleep apnea may be hyperactive and may be misdiagnosed with attention-deficit/hyperactivity disorder (ADHD).
Treatment-Non-surgical therapy
Continuous positive airway pressure is the nonsurgical gold standard. CPAP clearly reverses the apnea, stops the snoring, improves quality of life and sleep, and increases alertness. The downside is only 50% of people can tolerate the machine for any length of time. There are considerable technical issues that have to be overcome including the fitting of the mask or nasal pillows, sleep positioning, and the issues associated with the bed partner.
For those people that have mild apnea or snoring, conservative therapy is initiated first. This includes weight loss, avoidance of benzodiazepines (sleeping pills or muscle relaxants), and the use of alcohol before bedtime. A 10% weight loss is associated with a 26% decrease in the apnea-hypopnea index.
Since weight loss takes time and is only marginally successful for most people, other treatments are available. We work with a number of medical professionals in weight loss, nutrition, and exercise therapy to maximize our patients weight loss to achieve improvement. Oral appliances have been designed for individuals who are not surgical candidates and may have some undiagnosed craniofacial abnormalities that respond to oral appliances. These devices position the lower jaw, and modify the airway. Long term studies with oral appliances are lacking in the medical literature, and are clearly a suboptimal alternative to CPAP, however, for those without other alternatives oral appliances are a good solution. We also work with a number of dental professionals in our area who provide high quality services for our patients with sleep apnea.
Therapy-Surgical
Surgical therapy is directed towards the different levels of airway obstruction that
occur in sleep apnea. The airway from the nose to the larynx consists of the upper airway, and any place along this tract can have obstruction which may require correction. Additionally, the airway in sleep apnea must be reconstructed to both enlarge and tighten the tissues. Our approach is to first encourage patients to try CPAP. CPAP keeps the entire upper airway open using a positive pressure stream of air which opens the airway.
Nasal Airway Correction
If patients cannot tolerate the nasal CPAP device because of nasal airway obstruction, we proceed with nasal corrective surgery which may include a septoplasty, turbinate reduction with either a laser of radiofrequency device, and correction of nasal valves which become weakened with sleep apnea.
Nasal obstruction typically results in sleep disruption but contributes only a limited amount to sleep apnea. Patients with nasal obstruction and no sleep apnea have worse quality sleep. The purpose of correcting nasal abnormalities is to improve breathing quality at night, and allowing the use of nasal CPAP if patients have sleep apnea.
We utilize state of the art diagnostic testing in the office to determine the sites of nasal obstruction. Once determined, we offer the latest in radiofrequency turbinate reduction, minimally invasive septoplasty surgery, and balloon sinuplasty for patients with concomitant sinus problems. Dr. Kerner has developed procedures for correcting the nasal valves which when compromised, cause significant nasal obstruction.
Palate and Tonsil Surgery
The other airway levels that obstruct with OSA include the palate which we call the retropalatal (behind the palate) airway, and the retrolingual airspace (airway behind the tongue). The oral appliances can improve the retrolingual airway, but do little for the retropalatal airway. The palate contributes about 20% to sleep apnea, whereas, the retrolingual airway is responsible for approximately 80% of sleep apnea. Any surgical procedure must address all of these levels.
Surgery for the palate is very effective for snoring, but is only 50% effective for sleep apnea. This is because most people have retrolingual collapse in addition to retropalatal collapse, so surgery directed at the palate as the sole source of the problem is only partial treatment.
Procedures for the palate include a uvulopalatopharyngoplasty (UPPP), in which the soft palate is tightened, and tissue is removed to stiffen the palate. If tonsils are present, they are removed at the same time. For people with mild apnea and large tonsils we can approach this with radiofrequency technology. Dr. Kerner presented the largest series of minimally invasive tonsillectomy procedures at the American Academy of Otolaryngology meeting in September 2005. This is effective for reducing large tonsils and results in improved breathing and a reduction in throat infections.
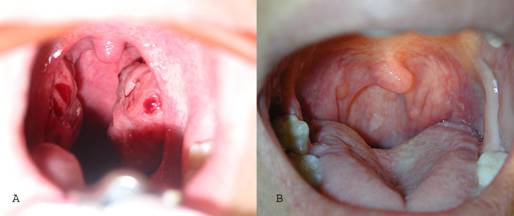
A-tonsils before radiofrequency B-Pharynx after radiofrequency tonsil reduction
When a palate surgery is indicated, Dr. Kerner utilizes the uvulopalatal flap. For patients with large tonsils, and a thick, elongated uvula, radiofrequency procedures are less effective so the more involved uvulopalatal flap with tonsillectomy is performed.
Tongue and Hypopharyngeal Procedures:
When there is evidence of retrolingual collapse (we determine this at the time of the initial examination using a flexible scope to evaluate the entire upper airway) other procedures are indicated to tighten and enlarge the retrolingual airspace. All of the procedures for the base of the tongue either tighten or enlarge this airway.
Radiofrequency devices are used to shrink the tongue; this requires multiple treatments and has been shown to be effective in reducing sleep apnea in a number of clinical trials.
A genioglossus advancement is a procedure that we have pioneered that creates a bone muscle flap with the primary muscle of the tongue, and repositions it through an incision in the mouth. [link to article on genioglossus and pdf article]
This creates a larger airspace and tightens the airway. We usually do this in conjunction with a hyoid-suspension myotomy which is a procedure that enlarges the airway behind the larynx. Multiple procedures can be done at the same time including palate surgery, tongue radiofrequency reduction, and genioglossus advancement/hyoid suspension myotomy.
For patients with skeletal deformities or severe apnea repositioning of the upper and lower jaws are sometimes indicated. This is what we term phase II surgery, and we reserve this for patients who fail phase I surgical procedures, and those with severe craniofacial abnormalities that require skeletal correction. Before these procedures are undertaken, special xrays called cephalometrograms, and panorex films are obtained. Sometimes a CT scan will be obtained for unusual airway findings. Some patients will require orthodonture to reposition the bite in the appropriate location.

Cephalometric radiograph
When multiple procedures are performed at the same we typically keep the patient overnight in the hospital for monitoring. When the procedures are done individually, they can be done safely on an outpatient basis.
The most important thing to understand is that sleep apnea is a complex disease that requires a proper diagnosis (physical examination and sleep study), and then an individualized treatment plan that begins with conservative therapy (weight loss, sleep positioning, oral devices, and CPAP.) When these treatments are inadequate, or not well tolerated, we then progress to more complex therapies. These include palate surgery, tonsillectomy, either with traditional techniques or with state-of-the-art radiofrequency tissue reduction techniques of the palate and tongue base. Phase 2 surgeries include jaw and tongue repositioning procedures, and craniofacial reconstruction procedures for more severe cases.
To Schedule a Consultation:
Call us at (818) 349-0600
We accept most insurance plans as out-of-network participants. Our staff can assist you with this prior to your consultation.
Bring as many past records that you have available, i.e. sleep studies, CT scans, X-rays, operative reports, and any other information that would helpful for us to make your visit as productive as possible.
The following are links to websites for more information:
www.entnet.org
www.sleepapnea.org
www.nhlbi.nih.gov/health/public/sleep/sleepapn.htm
www.airwaysurgfoundation.org